Most people in this space know the tryptophan trap. Serotonin gets hijacked. IDO flips on. Quinolinic acid builds up. Neuroinflammation follows.
But there’s a parallel story that doesn’t get nearly enough attention – and it runs straight through the sigma-1 receptor (Sig-1R).
Here’s why I’m investigating it.
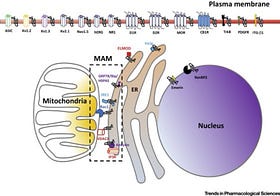
Sig-1R is a chaperone protein sitting at the ER-mitochondria interface. It regulates calcium handling, mitochondrial bioenergetics, and – critically – mast cell activation. When Sig-1R is underexpressed or dysfunctional, you lose a key brake on inflammatory signaling. Mast cells become more reactive. ER stress compounds. The gut-brain axis destabilizes.
Now add allopregnanolone to the picture.
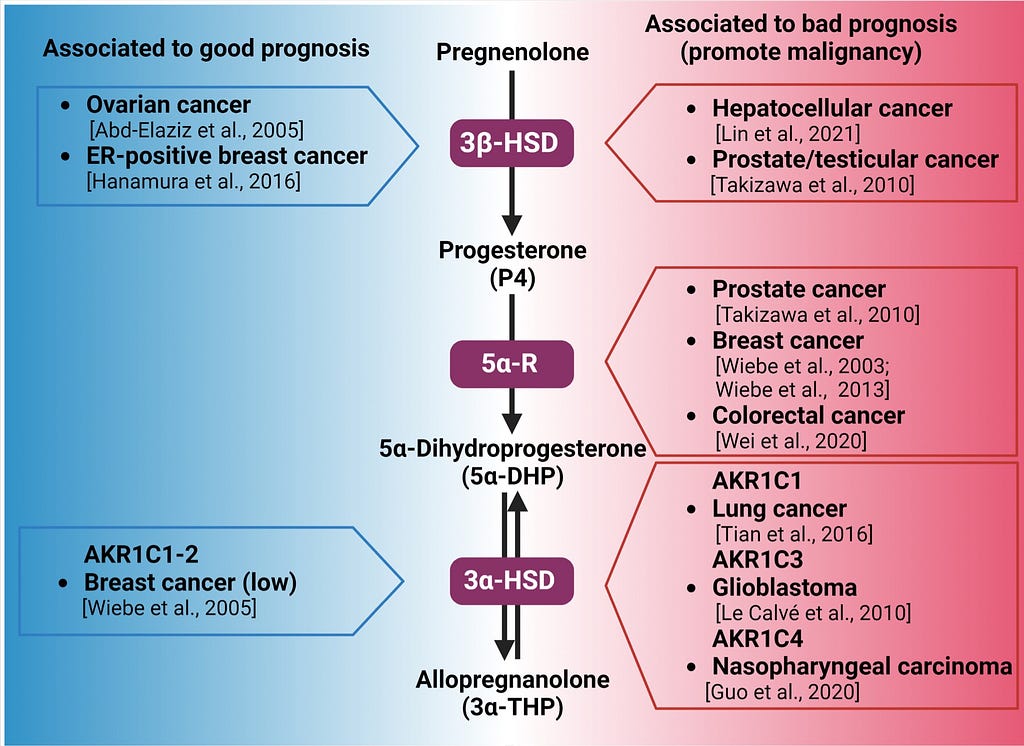
Allopregnanolone is a neurosteroid made from progesterone – it requires functional 5-alpha reductase (yes, genetics matter here, SRD5A2 variants included) and adequate progesterone substrate. It’s the brain’s endogenous GABA-A positive allosteric modulator. Calm. Anti-inflammatory. Neuroprotective.
But it’s also a Sig-1R ligand.
This is where it gets interesting. Allopregnanolone doesn’t just modulate GABA – it directly engages Sig-1R, influencing calcium signaling, mast cell tone, and mitochondrial resilience simultaneously.
Why I use the pregnancy model:
Pregnancy is one of the most controlled natural experiments we have. Progesterone surges. Allopregnanolone follows. Then delivery – a cliff drop. Postpartum depression isn’t just “hormones changing.” It’s a collapse of Sig-1R ligand availability, GABA tone, and neurosteroid-mediated mast cell regulation – all at once.
When I look at what changes in that window and who struggles most, I can start mapping the upstream vulnerabilities: 5-alpha reductase efficiency, receptor sensitivity to allopregnanolone, GABA-A subunit expression, and baseline mast cell burden.
This is also why MCAS symptoms so often flare postpartum, perimenstrually, and in perimenopause – same mechanism, different trigger.
I’m actively exploring whether targeted allopregnanolone support (through progesterone, 5-AR optimization, or receptor sensitivity work) may be a meaningful lever in MCAS, gut neuroinflammation, depression, and ADHD.
Have you noticed any improvement with progesterone, allopregnanolone, or neurosteroid-related support – especially postpartum, or during periods where your MCAS or gut symptoms shifted significantly?
Drop it in the comments. This thread is going somewhere. More on the neuroinflammation cascade to come.